MRU nursing across generations

Each spring, National Nursing Week invites Canadians to reflect on and recognize the impact of nurses. This year, the week runs from May 11 to 17 and is themed “The Power of Nurses to Transform Health.” Mount Royal University offers a powerful lens on that impact, one shaped by generations of nurses whose skill, compassion and leadership continue to transform care.
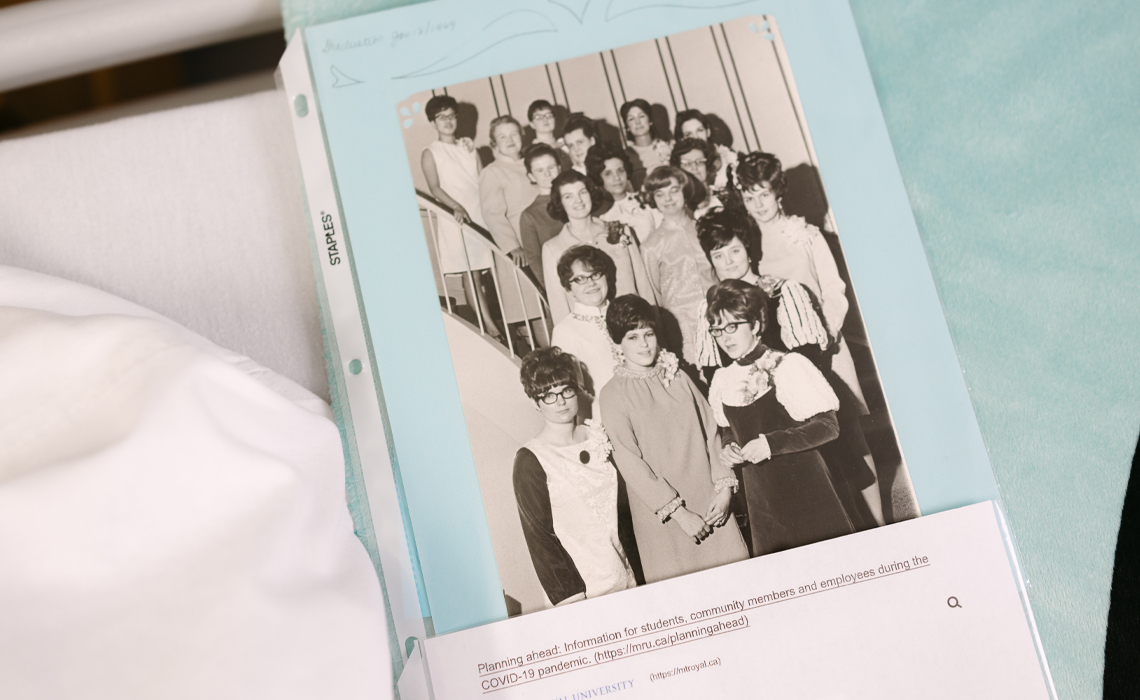
The legacy of MRU nursing alumni began in June of 1969, when the first class of nursing students received their diplomas at the Glencoe Club, nursing pins made of pure gold catching the light on their lapels. An all-female graduating class of 11, these bright young women stepped into a profession that would ask much of them — and shape even more in return.
Nearly 60 years later, Anne Kendrew of that same class sits across from two MRU nurses of different generations: Rachael Edwards (class of 2011) and Hamza Echchoujaa (class of 2026). The trio has returned to where it all began to share their stories: on campus, in the nursing lab, surrounded by ECG monitors and hospital beds that speak to how much has changed, and what has not.
Three generations of MRU nurses
Anne (Porter) Kendrew, a member of Mount Royal’s first graduating nursing class (1969) and 2020 Outstanding Alumni Award winner, transformed neonatal care in Calgary through compassionate innovation and determined leadership.

As manager of the Intensive Care Nursery at the former Holy Cross Hospital, she championed groundbreaking programs such as perinatal bereavement support, which allows parents to hold and say goodbye to their babies, and the Cuddlers program, ensuring hospitalized infants received vital human touch. Kendrew credits the extraordinary team around her, including doctors, nurses, social workers, clinical educators and volunteers, whose shared dedication made these initiatives possible.
Rachael Edwards, 2021 Outstanding Alumni Award winner and an alumna of the first Bachelor of Nursing cohort at Mount Royal (2011), has dedicated her career to supporting vulnerable populations through her work with CUPS Community Health Centre and the DOAP team.

In 2016, she co-founded the Calgary Allied Mobile Palliative Program, bringing accessible, dignity-focused end-of-life care to people experiencing homelessness. Edwards is also an active educator and is continuing her work to advance harm reduction and reduce stigma in health care.
Hamza Echchoujaa completed his nursing studies in December 2025 and will cross the stage this June as part of Mount Royal University’s class of 2026.

A dedicated leader in student health-care communities, he has served as president of the MRU Men in Nursing Club since 2022, fostering inclusion, mentorship and representation within the field.
Now a nurse with Alberta Health Services, Hamza has already been recognized for his impact, receiving both a Students’ Association of Mount Royal University award and the Alberta Immigrant Impact Award (Young Leader category). His leadership and commitment to community continue to shape his growing career in nursing.
Edwards »
For me, even the term ‘vulnerable populations’ can be a bit triggering, because I don’t think of the people we work with as inherently vulnerable. We’re all people. We don’t all carry the same risks, but vulnerability isn’t something that simply exists within individuals.
Our systems create it.
When certain groups are excluded or marginalized, they become more vulnerable to poor health outcomes. It’s not just the health-care system. Many of our systems contribute to this. They create conditions that wouldn’t otherwise exist, pushing people to the margins.
As nurses, we work with diverse populations everywhere we go. Alberta is incredibly diverse, and that shapes the kind of care we provide.
In the literature, ‘vulnerable populations’ are often described as those at higher risk of poor outcomes due to factors like age or disability. For example, the very young or the very old may be more susceptible to illnesses like influenza. But more broadly, the term is used for people who don’t have equal access to the social determinants of health.
When access to those determinants is uneven, people experience worse outcomes. That can be tied to race, gender, socioeconomic status or other factors. In practice, we care for people across all of those categories. People living in poverty, people who use substances, people with disabilities and people who are immunocompromised.
They’re often labelled as vulnerable. But I tend to focus on the system side of it. In the last few years after COVID, we're losing more and more and more community health nurses.
Kendrew »
When I think back on my years in the North, working on reserve, I remember the people I met there. Many became very dear to me. They were living in poverty, and at that time, in the early 1970s, health care in the North was run by the Catholic Church. It has since been taken over by Northern Health, with more government support and resources, but back then, there was very little.
There was no social assistance. We didn’t have social workers. Support systems were limited, although families did their best to take care of one another, which made a difference.
I remember many nights when people would come in after drinking, and there was nowhere for them to go, nowhere at all. It was either the jail or the hospital. And I only had one hospital bed, which I was supposed to keep available.
One night, it was 30 below, and the doctor told me to send someone away. He said, ‘Let them go.’ But I knew they would freeze to death. I said, ‘I’m admitting them.’ I remember thinking I might lose my job in the morning.
I didn’t. And when I asked the doctor later what he would have done, he said, ‘I would have admitted them too, even if we had to put them on the floor.’
That experience in the North stayed with me.

Kendrew »
In those days, parents were not allowed to be with their premature or sick children. I was working as a candy striper (volunteer) at the children's hospital, and there was a baby, maybe a few months old, crying. I asked the nurse if I could cuddle this baby, and as I was holding her, I thought, there is something wrong. It turned out she was blind, and all I could think of was that poor little thing crying, all on its own. That would seem like a prison. And I thought, I've got to be a nurse. I have to work with little ones and children and make sure that we can get parents in with them.
Echchoujaa »
My youngest brother was born with tetralogy of Fallot, so he had four heart defects and needed a couple of open-heart surgeries. From a really young age, I was exposed to the health-care environment.
I remember rooming in with him after one of his surgeries and watching how the nurses cared for him. I was still just a kid, but it made a huge impression on me. You know, the surgeons felt larger than life, but it was the nurses who were there for everything else. They managed his pain, watched for complications and handled every issue that came up.
They were also so kind and engaging. They would involve me in little ways, just enough to distract me because I was scared and emotional. Looking back, I can see how intentional that was.
That experience really drew me to nursing. I knew I wanted to do that for other people. I wanted to support families who are struggling, who are in pain and help improve their outcomes.
By the time I got to high school and started thinking about my future, it felt clear. Nursing was the only path I could see. And since then, every class, every clinical, every shift has only reinforced that decision.
Edwards »
I was a dental assistant before I became a nurse, and I really loved dentistry. But there wasn’t a degree pathway in that field, and I knew I wanted to go further. I was also interested in research, but I didn’t want to lose that connection with patients.
When I moved to Calgary from Victoria, I started volunteering at the dental clinic at CUPS. They serve people living in poverty, people experiencing homelessness and people who use substances. And that was the first place in Alberta where I felt at home.
At that point, it became clear. Nursing was the path, and that was the population I wanted to work with.
I went into nursing thinking I probably wouldn’t work in a hospital, and I didn’t. I stayed at CUPS from the time I graduated until 2018. I feel really fortunate to have found that passion so early on.
Nursing just became a natural extension of that work. And one thing that’s always stayed true for me is that we learn far more from our patients than they ever learn from us.
Kendrew »
The biggest thing I never would have foreseen is the extent of computer use. Computers were only beginning to enter practice when I retired, so I never had to work with them in the way nurses do now. We ran around with a piece of paper in our pockets, recording vital signs and tasks, and then charted everything at the end of the shift.
I also miss back rubs and foot care. During a bed bath, we soaked feet, gave back rubs and assessed the patient while providing comfort. Back rubs helped patients sleep, and they gave nurses energy, too. Nurses of my generation often miss that aspect of care.
Edwards »
I remember paper documentation, too, so electronic systems are not that far removed from my own experience. We have digitized so much. On one hand, electronic records help us access information from across the province, which can improve care when people are vulnerable or unable to give a full history.
On the other hand, diagnoses follow people. If someone has ever been diagnosed with opioid use disorder, that information may appear immediately in the chart and influence how they are treated. HIV is another example. Today, HIV is a chronic illness and is often easier to treat than diabetes, yet it can still appear as an alert and create stigma. Not every health-care professional needs every piece of information, and patients should have more control over disclosure than our systems allow.
Electronic records can also reveal that someone has accessed a supervised consumption site. If that person later comes to the emergency with legitimate pain, that history may bias the care they receive.
When computers go down, we miss paper charts because we knew where everything was. Downtime is very challenging.
Echchoujaa »
I have used paper charts during downtime. Once, Netcare went down for several days, and everything was backlogged. In a high-acuity area, you can only imagine how thick my stacks of notes were.
Those moments show why older skills still matter. Manual blood pressure is a good example. Machines fail, batteries die, or equipment is not calibrated. Once, when I was an undergraduate nurse, a patient became septic, and the automatic machine could not read the blood pressure. I had to take it manually. We keep evolving, but the foundations remain.
Now we are facing another major shift with artificial intelligence. In situations where patients are intubated or unconscious, a level of automation makes sense. Still, there’s a concern about how far it could go. Could we reach a point where nurses rely so heavily on technology or AI that full patient assessments become less common? It’s a delicate balance, and we have to be thoughtful about how much responsibility we hand over to these systems.
Echchoujaa »
During my preceptorship in the emergency department, a young man came in from a reserve after being attacked by a dog. He had serious injuries and was in excruciating pain.
But when we tried to give him pain medication, he refused.
It turned out his brother had gone through something similar. He had been neglected and given the wrong medication, which unfortunately led to his death. So for him, that distrust wasn’t just a feeling. It was a lived experience.
And you realize this isn’t a one-time thing. It happens again and again, and it creates a deep mistrust of the health-care system and of us as providers.
So for me, that changed how I approach care. I take more time. I explain everything in detail — what the medication is, what it does, what to expect, possible side effects, and what we’ll do if something goes wrong. You go deeper than you normally would, because you’re trying to build that trust.
Rapport is always important in nursing, but in these situations, you have to go even further. You have to give people time, time they haven’t always been given.
You can’t undo what’s happened in the past. But you can try to make sure their experience with you is the best it can be.
Because otherwise, they won’t come back. And when that happens, something treatable can become life-threatening. An infection can turn into sepsis. An injury can cost someone a limb.
So a big part of my role is advocating for that, making sure people feel safe enough to trust the care they’re receiving.
Kendrew »
I’ll try to keep this short, because it’s really one of my favourite parts of my career. The Cuddlers program.
At the time, we were working in the intensive care nursery, and these babies needed more care than we could give. Parents couldn’t always be there, and some of these little ones were in the unit for months. We knew they needed that human touch.
So we decided to start a volunteer program. I went to the chief of pediatrics, and he said, ‘It’s a wonderful idea, we need that. But the administrator will never approve it.’ I said, ‘Okay, I’ll go talk to him.’ And he said, ‘You will?’ I said, ‘Yes.’
So I took my director down, and the administrator said the same thing in reverse. ‘Lovely idea, but the chief would never go for it.’ So we had them. And that’s how it started.
We worked with volunteer services and launched the program. We put out a call in the Calgary Herald and received about a thousand applicants. We only brought on eight or nine to start. It was a pilot, so we trained them carefully, made sure staff and families were comfortable, and always had them working alongside a nurse. It was a wonderful program. We published it in The Canadian Nurse, and before long, hospitals across the country were starting their own.
And then, alongside that, we began changing how we cared for families who lost babies.
At the time, parents weren’t allowed to see or hold their child. The belief was that they shouldn’t grieve the loss of a baby in that way. But we knew that wasn’t right. That relationship begins long before birth.
So we changed it. We made sure parents could hold their baby, spend time and say goodbye.
That was just as important.

Thank you to our guests, Anne Kendrew, Hamza Echchoujaa and Rachael Edwards for sharing their stories in honour of National Nursing Week. Their reflections offer more than a glimpse into their lives; they reveal the compassion, heart and humanity at the core of nursing.
The impact of Mount Royal nurses extends far beyond individual journeys. It lives in the quiet moments of care, in the courage to challenge systems, and in the commitment to show up for patients and communities every day.